|
|
 ? ?  ? ? |
| ORIGINAL ARTICLE |
|
|
Year : 2012? |? Volume : 1? |? Issue : 2? |? Page : 74-78 |
|
Impact of socioeconomic status on decayed, missing, filled teeth (DMFT) among state government employees in Shimla City, Himachal Pradesh
Vinay Kumar Bhardwaj1, Koratagere Lingappa Veeresha2, Kapil Rajiv Sharma3
1?Department of Public Health Dentistry, H.P. Govt. Dental College and Hospital, Shimla, Himachal Pradesh, India
2?Department of Public Health Dentistry, Maharishi Markandeshwar College of Dental Sciences and Research, Mullana, Haryana, India
3?Department of Paediatric and Preventive Dentistry, H.P. Govt. Dental College and Hospital, Shimla, Himachal Pradesh, India
| Date of Submission |
23-Jun-2012 |
| Date of Acceptance |
02-Dec-2012 |
| Date of Web Publication |
8-Jan-2013 |
Correspondence Address:
Vinay Kumar Bhardwaj
Department of Public Health Dentistry, H.P. Govt. Dental College and Hospital, Shimla, Himachal Pradesh
India

DOI: 10.4103/2278-9588.105674

Objectives: To assess the impact of socioeconomic status (SES) on decayed, missing, filled teeth (DMFT) among state government employees in Shimla city, Himachal Pradesh.
Design: Cross-sectional study.
Materials and Methods: This study was conducted on 1008 dentate subject 705 (69.9%) males and 303 (30.1%) females out of 10908 government employees. Data regarding dentition status and treatment needs was recorded on a W.H.O. format 1997. Type III examination was conducted under good illumination by the investigator himself. Student's t-test or ANOVA was applied for statistical evaluation of means and the comparisons of proportions. P value ? 0.5 and ? 0.01 was considered statistically significant and highly significant respectively.
Results: Total teeth examined were 29575 out of which 14.84% were decayed. Overall mean DMFT was 3.29 (1.86). Females were reported significantly higher ( P < 0.05) DMFT 3.49 (2.31) than males 3.12 (1.42). Subjects who belong to upper SES had lesser mean DMFT than lower SES 2.31 (2.4) vs 4 (3.89), which was statistically highly significant ( P < 0.01). Employees who brush their teeth once a day presented with higher DMFT 4.01 (2.01) than those who brush once daily 2.57 (1.96). The difference was highly significant ( P < 0.01).
Conclusions: A preventive and curative oral health policy for the government employees in Shimla city needs to be planned and implemented to maintain their commitment in their official work. Also they must be educated the importance of oral health and methods how to maintain it.
Keywords:?Decayed, filled teeth, government employees, missing, socioeconomic status
How to cite this article:
Bhardwaj VK, Veeresha KL, Sharma KR. Impact of socioeconomic status on decayed, missing, filled teeth (DMFT) among state government employees in Shimla City, Himachal Pradesh. J Cranio Max Dis 2012;1:74-8 |
How to cite this URL:
Bhardwaj VK, Veeresha KL, Sharma KR. Impact of socioeconomic status on decayed, missing, filled teeth (DMFT) among state government employees in Shimla City, Himachal Pradesh. J Cranio Max Dis [serial online] 2012 [cited?2013 Aug 27];1:74-8. Available from:?https://craniomaxillary.com/text.asp?2012/1/2/74/105674 |
|
??Introduction |
? |
 |
Health is a state of complete physical, mental and social well being of a person and doesn't merely absence of a disease or infirmity. [1] Oral health is an integral part of general health. Loss of teeth substantially reduces the quality of life. [2] Oral health is mainly determined by the prevalence of dental caries and periodontal disease, the former being one of the most widespread chronic diseases in the world. [3] Dental caries can aptly be termed as a scourge of modern civilization and no nation, continent or race has escaped the ill effects. Socioeconomic status (SES) plays a vital role in its determination. [2] State government employees, who are the backbone of government machinery in Shimla, have free access to oral health care facility. Government employees do have health care privileges such as paid holidays for the medical and dental care, reimbursement of cost of denture being fabricated at government hospital or at recognized private hospital. [4] With all these facilities they are supposing to having better dentition status. Voluminous literature exists on the oral health status and treatment needs among different populations in India and worldwide, [5],[6],[7],[8],[9],[10] but there is no data on the dental caries and its relationship with SES among the state government employees in Shimla city. Hence this study has been taken up to assess dentition status of these employees in Shimla city and the influence of SES and other variables on it. Results of this study will be very important for establishing priorities and determining the type and quantity of preventive and interceptive services required and to extend more facilities for dental care.
|
??Materials and Methods |
? |
|
This cross sectional study was conducted on state government employees in Shimla. Being capital of Himachal Pradesh, Shimla harbors the head offices of all the departments. Total number of state government employees in Shimla city was 10908. [11] Official permission was obtained from the heads of all the departments and an ethical approval from the institutional ethical committee. Cross sectional study was conducted on 1008 dentate subjects out of 10908 government employees. A proportionate sample was taken from each department and cadre. The criteria for inclusion were any employee of the state government of Himachal Pradesh posted in Shimla headquarters, who were dentate and were willing to participate in the study. The criteria for exclusion were any disease or ailment that could affect or cause deterioration in the subject's general health and oral health problems; and those who were edentulous. Informed consent was obtained from all those who were examined. Modified Kuppuswamy scale, [12] with readjustment of the per capita income to suit the present levels was used for classifying the individuals into one of the five socio economic categories. Data regarding dentition status and treatment needs was recorded on a modified W.H.O. format 1997. [13] Type-III examination as recommended by American Dental Association which includes inspection using a mirror and probe under good illumination was conducted. [14] The recorder was asked to sit close to the investigator. Clinical examination was done using a mouth mirror and a CPI probe. The data was collected by single examiner between 25 th February 2009 and 10 th April 2009.
The examiner was first calibrated against an experienced examiner to ensure the reliability and validity of the results. The percentage agreement for dentition status was 98.9% and the Kappa value was 0.85. To ensure consistency throughout the study, a random of 10% of the sample was re-examined and the intra-observer agreement was 99% and the kappa value was 0.89 for the same. Each examination session was followed by dental health education to the employees. The needy were issued referral cards and motivated to seek treatment at government dental college and hospital on priority basis.
The data were analyzed using the software Statistical Package for the Social Sciences version 15 (SPSS Inc., Chicago). Frequency distributions were used to describe the data; means of decayed (D), missing (M) and filled (F) permanent teeth (T) were calculated. The Student's t-test or ANOVA was applied for statistical evaluation of means and the comparisons of proportions. P value ? 0.5 and ? 0.01 was considered statistically significant and highly significant respectively.
|
??Results |
? |
|
Study sample consists of 1008 subjects out of which 705 (69.9 %) were males and 303 (30.1%) were females with a mean age 41.35 ? 8.31 years. All the subjects in the study were divided into five groups i.e., 18-24, 25-34, 35-44, 45-54 and 55-58. Maximum subjects were in the age group of 35-44 years while minimum were in the 18-24 years age group [Table 1]. Overall DMFT among males and females was 3.12 (1.42) and 3.49 (2.31) respectively. Highest DMFT 4.12 (2.13) was observed in the age group 35-44 years in contrast to the lowest DMFT 1.94 (0.93) in the youngest age group. Females were having higher DMFT than males. For all age groups the 'D' component constituted major proportion of the caries index [Table 2]. Sample was divided into five SES categories in which maximum employees belong to lower middle class whereas only one employee belong to the lower SES category. SES categories were inversely associated with mean DMFT [Table 3]. Out of the whole sample 539 (53.47%) brushed their teeth twice daily whereas 469 (46.53%) brushed only once. Mean DMFT of those subjects who brush their teeth once a day was higher than those who brush twice daily 4.01 (2.01) vs. 2.57 (1.96) [Table 4].
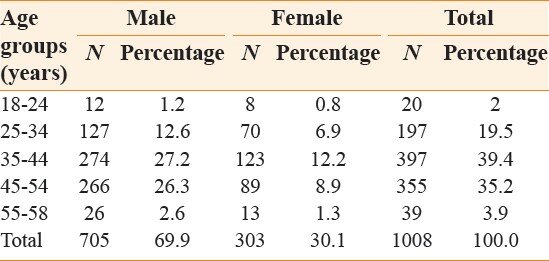 |
Table 1: Age wise and gender wise distribution of the subjects
Click here to view
|
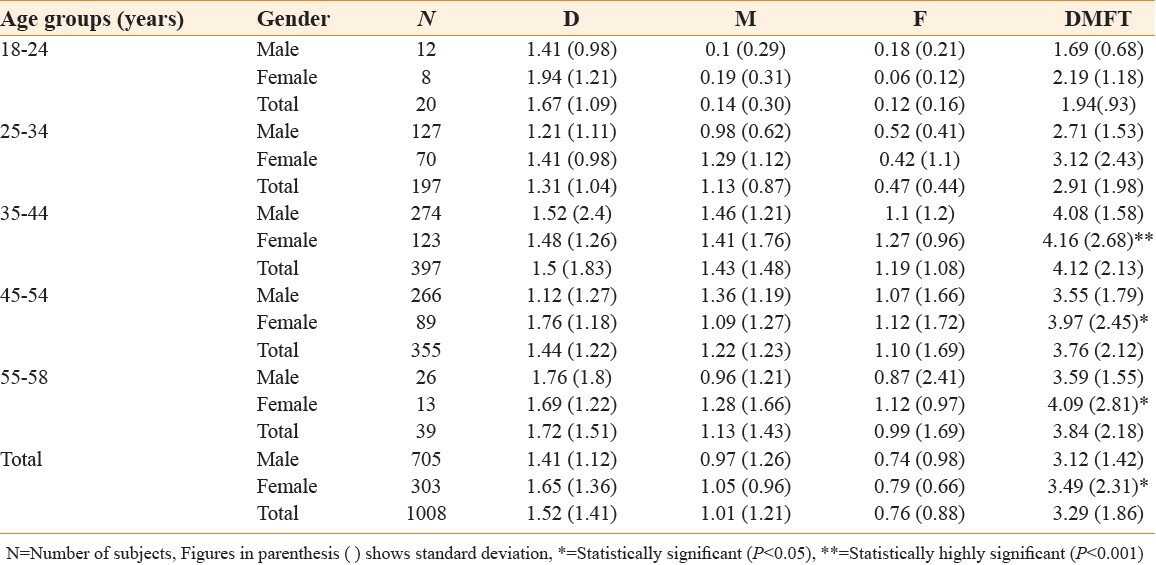 |
Table 2: Mean DMFT, age wise and gender wise
Click here to view
|
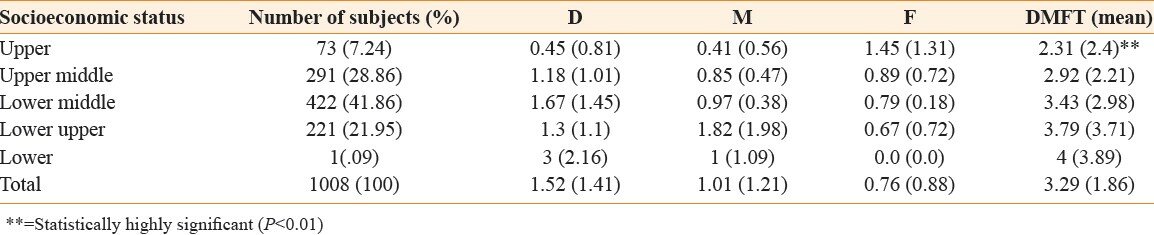 |
Table 3: The mean DMFT in relation to socioeconomic status
Click here to view
|
 |
Table 4: Mean DMFT in relation to frequency of brushing
Click here to view
|
|
??Discussion |
? |
|
This study was conducted to provide data on the dentition status of the state government employees in Shimla city in Himachal Pradesh and its association with socioeconomic variables and oral hygiene practices. The outcome would aid in planning and extending more facilities to these employees. The epidemiological data was collected according to the WHO standard method and criteria. The recording included dental caries and treatment needs which are highly relevant conditions in planning oral health programmes.
The employees were between the age of 18 years to 58 years which is the age of recruitment and superannuation in Himachal Pradesh.
Number of sound teeth present was 84%.This reflects the awareness of the employees about the maintenance of oro-dental health. Mean DMFT increases upto the age group 35-44 years and then decreases. Increase in the mean DMFT in this age group may be due to cumulative effect of different diseases. Mean DMFT irrespective of the gender was 3.29 (1.86). Similar findings were reported by Frencken et al. [15] and Varenne et al. [16] Contrasting higher DMFT was reported by Vrbic et al. [17] in their studies and lower DMFT was reported by Wang et al. [18] in China. This difference may be attributed to different geographical, ethnical and cultural variations, fluoride contents of drinking water. DMFT values showed an increase up to the 35-44 years age group. This may be attributed to the more missed teeth and removal of teeth in the older age groups. Among different age groups in this study, highest DMFT was observed in the age group of 35-44 years and lowest in the 18-24 years age group. Females were reported having significantly higher DMFT than males. This gender wise comparison was significant in the age groups 45-54 and 55-58 years (P < 0.05) and highly significant in the age group of 35-44 years (P < 0.001). Cortes et al., [19] Petersen et al., [20] and Madlena et al. [21] had also reported similar results.
Socioeconomic status took into account (education status, occupation and income) [12] of the subjects. Socioeconomic status had shown an inverse relationship with the mean DMFT similar to the findings reported by Corbet EF [22] and Doifode et al. [8] Upper category had the lowest DMFT 2.31 (2.4) while the lower category had the highest DMFT of 4 (3.89). 'F' component was higher among the employees of upper SES than 'D' component, whereas for lower SES employee 'D' component was higher than 'F' component. This shows that the treatment availed by upper SES class was more than lower SES class which shows their awareness towards maintenance of oral health. The reason may be that, lower educational status, primitive idea about oral hygiene and not availing the preventive and curative facility by the lower SES category. Sathpathy [23] in his study on police personnel, Garre et al. [24] in a study on Indonesian soldiers and Timis [25] had revealed similar findings.
Better oral hygiene practices were found to be associated with lower prevalence of dental caries similar to the findings of Doifode et al. [8] Frequency of tooth brushing had shown an inverse relationship with mean DMFT values. Those subjects who were brushing once daily had higher DMFT 4.01 (2.01) than those brushing twice daily 2.57 (1.96). The difference was highly significant (P < 0.001). This could be due to more cleansing of the teeth and better oral hygiene resulting into lesser decay of teeth.
|
??Conclusion |
? |
|
Inequalities in socioeconomic status underlie many health disparities in the world, including oral health. Most of the dental health services provided to the government employees in Shimla city; Himachal Pradesh, have been treatment oriented. Therefore efforts need to be focused above all on raising this population's awareness of the importance of oral hygiene, regular dental checkup for early diagnosis of dental caries and treatment at well established dental care centers in government sector as well as authorized private clinics in Shimla city. To meet this objective, a preventive and curative oral health policy for the government employees in the state of Himachal Pradesh, defining resources, objectives and priorities, needs to be planned and implemented.
|
??Acknowledgement |
? |
|
I thank all the government employees who agreed to take part in this study. I also thank government dental college administration, staff in the department of public health dentistry, statistician and head of the department of the concerned government offices.
?
|
??References |
? |
|
| 1. |
Park K. Concept of Health and Disease. Park's text book of preventive and social medicine; 20 th ed. Jabalpur India: M/S Banarsidas Bhanot publishers; 2009. p. 12-48.??
???? |
| 2. |
Slade GD, Spencer AJ. Social impact of oral conditions among older adults. Aust Dent J 1994;39:358-64.??
[PUBMED]???? |
| 3. |
Aleksejuniene J. Caries experience and oral hygiene in Lithuanian children and adolescents. Acta Odontalgia Scandinavia 1996;54:75-8.??
???? |
| 4. |
Muthuswamy P, Bindra V. Swamy's Handbook 2009 Orders Based on Sixth Pay Commission Recommendation. 35 th ed. Chennai: Swami Publishers (P) Ltd; 2009.??
???? |
| 5. |
Mosha HJ, Ngilisho LA, Nkwera H, Scheutz F, Poulsen S. Oral health status and treatment needs in different age groups in two regions of Tanazania. Community Dent Oral Epidemiol 1994;22:307-10.??
[PUBMED]???? |
| 6. |
Petersen PE, Razanamihaja N. Oral Health status of children and adults in Madagascar. Int Dent J 1996;46:41-7.??
[PUBMED]???? |
| 7. |
Petersen PE, Tanase M. Oral health status of an industrial population in Romania. Int Dent J 1997;47:194-8.??
[PUBMED]???? |
| 8. |
Diofode VV, Ambadekar NN, Lanewar AG. Oral health status and its association with some epidemiological factors in population of Nagpur, India. Indian J Med Sci 2000;54:261- 9.??
???? |
| 9. |
Dougan B, Kassak K, Bourgeous DM. Oral Health Status and treatment needs of 35-44-year old adults in Lebanon. Int Dent J 2000;50:395-9.??
???? |
| 10. |
Mandal KP, Tewari AB, Chawla HS, Gauba KD. Prevalence and severity of dental caries and treatment needs among population in the eastern states of India. J Indian Soc Pedodont Prev Dent 2001;19:85-91.??
[PUBMED]???? |
| 11. |
51 st Census of government employees in Himachal Pradesh as on 31.3.2008 department of economics and statistics, Government of Himachal Pradesh.??
???? |
| 12. |
Kumar N. Kuppuswamy socioeconomic status scales - updating for 2007. Indian J Pediatr 2007;74:1131-2.??
[PUBMED]???? |
| 13. |
World Health Organization. Oral Health Surveys, Basic methods, 4 th ed. Geneva; 1997. p. 26-9.??
???? |
| 14. |
Thilender B, Seeman L, Ingervall B. Prevalence of malocclusion and orthodontic treatment need in children and adolescent in Bogota, Colombia. An epidemiological survey related to different stages of dental development. Eur J Orthod 2001;23:153-67.??
???? |
| 15. |
Frencken JE, Rugarabamu P, Amuli JA, Mulder J, Lihepa A. Oral health status of employees in sugar and sisal estates in Tanzania. Afr Dent J 1989;3:9-16.??
[PUBMED]???? |
| 16. |
Varenne B, Petersen PE, Seydou O. Oral health status of children and adults in urban and rural areas of Burkina Faso, Africa. Int dent J 2004;54:83-9.??
???? |
| 17. |
Verbic B, Homan D, Zavrshik B. Oral Health in Slovania, Yugoslavia. Community Dent Oral Epidemiol 1991;19:72-3.??
???? |
| 18. |
Wang HY, Petersen PE, Bian JY, Zhang BX. The second national survey of oral health status of adults in China. Int Dent J 2002;52:283-90.??
[PUBMED]???? |
| 19. |
Cortes FJ, Moreno C, Arandez E. Tooth loss and dental caries in adult population in Navarra, Spain. Community Dent Oral Epidemiol 1993;21:72-3.??
???? |
| 20. |
Petersen P E, Kaka M. Oral Health status of adults in the Republic of Niger, Africa. Int Dent J 1999;49:159-64.??
???? |
| 21. |
Madlena M, Hermann P, Jahn M, Fej?rdy P. Caries prevalence and tooth loss in Hungarian adult population: results of a national survey. BMC Public Health 2008;21:364-9.??
???? |
| 22. |
Corbet EF. An international comparison of socio-economic status and oral health. Br Dent J 2003;88:194.??
???? |
| 23. |
Satapathy DM, Behera TR, Tripathi RM. Health status of traffic police personnel in Brahamapur city. Indian J Community Med 2009;34:71-2.??
[PUBMED]?? ?? ?? |
| 24. |
Gaare D, Joelimar FA, Ouderaa FV. A cross-sectional study of DMFT and CPITN scores in a group of Indonesian soldiers. Eur J Oral Sci 1989;97:20-4.??
???? |
| 25. |
Timis T, Danila I. Socioeconomic status and oral health. J Prev Med 2005;13:116-21.??
???? |
?
?
? [Table 1], [Table 2], [Table 3], [Table 4]
|
|
| ? |
|
|







 ??Search Pubmed for
??Search Pubmed for
